[English version below]
Llaman a la puerta y voy a abrir. Es mi hija pequeña, agitada y angustiada como nunca. Entra, no se quita la mascarilla pero me abraza. Cosa rara, siempre se quita la mascarilla en casa. Es un abrazo intenso, como si fuera a acabarse el mundo. Llora. Le acaricio la espalda. Se calma y puedo hablarle mientras entramos en el cuarto de estar y nos sentamos.
-Hija, no hay nada que me preocupe más que verte así, rota.
-Mamá, es que me han dado el resultado del análisis que han hecho a todos los profesores, ya sabes, y dicen que ahora tengo que hacerme la PCR, esa prueba que sólo entendí cuando tú me lo explicaste.
-Sí. Lo de la Comunidad Autónoma de Madrid ha salido en todos lados, lo de las colas interminables. Dicen que quieren hacer las pruebas serológicas a 100.000 personas relacionadas con la educación como parte de su estrategia para un inicio seguro de curso 2020/21.
-Pues eso. No te quería molestar así que fui cuando me citaron y tuve la suerte de ser de las primeras. Pero ahora me han dado el resultado y estoy hecha un flan, no me tengo. He dado positivo para IgM y negativo para IgG. Y en este papel que nos han dado pone literalmente “Infección aguda. Recibirá una citación en 24 horas para la realización de la PCR”.
-¿Y te han llamado?
-No. Así que he intentado llamar a donde nos lo hicieron sin éxito. Y tampoco me han atendido en el centro de salud, ni la enfermera ni el médico, el teléfono está bloqueado. Por eso he venido a verte, desquiciada, perdona. No soy capaz de esperar un día a que me llamen. Esto es lo mejor que he encontrado en Internet.

-¡Te puedes imaginar cómo estamos, no paran de llamarme compañeros preguntándome a mí, con eso de lo que escribiste sobre la PCR! Y en los grupos corren todo tipo de interpretaciones. ¡Es para volverse loca! No sé a quién se le ocurriría, pero ha metido la pata.
¿Te notas algo, estás bien?
-¡Mamá! Estoy como una rosa, claro, sí, preocupada con el comienzo del curso y todo el lío que nadie aclara. Ya sabes, habían dicho que iban a contratar a 11.000 profesores nuevos y al final son sólo 300 ¡y con el contrato sólo hasta Navidades!
-Son unos sinvergüenzas. Pero, y Jorge ¿también está bien? Que yo sepa le dieron el alta y la PCR fue negativa, ¿no?
-Sí, sí, está muy bien desde el alta, hace ya casi tres semanas.
-Y no has tenido contacto con nadie más que haya sido diagnosticado ni aislado por covid, ¿es así?
-Sí, sí, con nadie.
-Entonces, si no has tenido contacto con nadie infectado y/o enfermo y si estás bien (sin fiebre, ni tos, ni agobio al respirar, ni catarro, ni pérdida de olfato, ni cansancio, ni dolor muscular, ni nada de nada) sería raro que estuvieras infectada. Es probablemente un falso positivo. ¿Quieres que te lo explique?
-Vale, sí, mamá.
-Son varios puntos seguidos, si entiendes el primero seguro que entiendes el siguiente, y así sucesivamente:
- Los seres vivos responden a las infecciones de muchas maneras, pero una de ellas es con lo que la gente llama “defensas”, los anticuerpos.
- Los anticuerpos son proteínas que llamamos inmuno-globulinas, y de ahí la abrevitura de “Ig”.
- Su estructura es increíble, una maravilla de la Naturaleza, pero lo fundamental es que tienen un extremo muy variable, apropiado a cada antígeno (parte del germen que provoca la formación de los anticuerpos) y hay millones de extremos distintos, y por ello millones de anticuerpos diferentes, adaptados a los múltiples antígenos.
- Cuando una persona se infecta con el nuevo coronavirus, SARS-CoV-2 se producen anticuerpos para defendernos de la infección (inmuno-globulinas anti SARS-CoV-2).
- Se pueden medir en sangre los anticuerpos específicos para el nuevo coronavirus, tomando una muestra como te han hecho a ti, con una técnica que llamamos ELISA y a veces con otras más rápidas.
- Se pueden medir el conjunto, anticuerpos totales (Igt), o algunos más específicos, A, M y G (inmuno-globulinas IgA, IgM, IgG). Si hay prisas, lo más rápido y seguro es medir las inmunoglobulinas totales (Igt).
- En general se prefiere identificar las IgM y las IgG porque hay menos errores.
- Las inmunoglobulinas IgM son anticuerpos de aparición temprana (al poco de la infección, en torno a 7 días después del contagio) y las inmunoglobulinas IgG son anticuerpos de aparición tardía (en torno a los 12 días después del contagio) y persistentes en el tiempo (no se sabe todavía, pero meses en general).
- Ya sabes cómo somos los seres vivos, tan variables, así que a veces la producción de anticuerpos es casi inapreciable, pero puede haber otras defensas, como las de los células T. En general, en las personas infectadas pero que no desarrollan síntomas, que no tienen la enfermedad “florida” (la pasan, pero es inaparente), la produccion de anticuerpos es más débil y esos anticuerpos duran menos tiempo en la sangre.
- “¿Me sigues?”
- “Sí, mamá. Es muy sencillo, me han medido dos anticuerpos en sangre contra el coronavirus, las inmunoglobulinas M y G, porque son los que dan menos errores. Las M son las primeras que aparecen en la sangre, y luego las G. Si me infecto y no tengo síntomas produzco menos anticuerpos y duran menos en la sangre”
- “Vale, sigo”.
- El nuevo coronavirus es un virus especial en cien formas, incluyendo que no se cumple tan rigurosamente la cadencia de anticuerpos. En general se forman primero las IgM, como respuesta temprana, y al cabo de los días se forman las IgG, pero en este caso no es tan claramente así.
- A veces no se pueden determinar en sangre hasta dos semanas después del comienzo de los síntomas, y se elevan al tiempo las dos inmuno-globulinas, IgM e IgG, o aumentan incluso primero las IgG.
- En los anticuerpos contra el nuevo coronavirus hay una inconsistencia en la aparición de ambas clases de anticuerpos y es un poco absurdo interpretar la IgM como «temprana», que es lo que suele hacerse en muchas otras infecciones. Por eso es todo más complicado, y todavía más cuando no hay síntomas de enfermedad ni sospecha clínica de la misma de forma que la detección de anticuerpos termina siendo totalmente inútil.
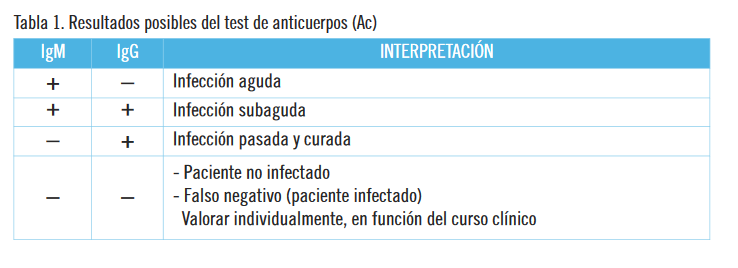
- En general, no obstante, se suele interpretar que una persona que tiene anticuerpos ha sido infectada por el virus, y 1/ si tiene sólo las inmuno-globulinas tempranas (IgM), que está en las primeras fases de la infección, 2/ si tiene las dos (IgM e IgG), que está en fase de infección avanzada, 3/ si sólo tiene las inmuno-globulinas tardías (IgG), que pasó la infección y tiene defensas, y 4/ si no tiene ningún anticuerpo, ni IgM ni IgG, que no ha tenido contacto con el virus.
- Esta formación de anticuerpos se da tanto en personas que han tenido síntomas y la enfermedad COVID19 como en personas que se han contagiado y han superado todo sin dar síntoma alguno.
- En todo caso, te puedes imaginar que no hay prueba médica “exacta”, ni existe ninguna prueba científica que no tenga sus limitaciones.
- Es decir, que la prueba puede dar resultados falsos, en los dos sentidos, falsos positivos y falsos negativos.
- En realidad, la determinación de anticuerpos es para el diagnóstico, cuando hay síntomas y sospecha clínica de enfermedad, no para personas sin síntomas. Y son tests que todavía no se han perfeccionado en el sentido clínico, y menos en personas asintomáticas.
- Las características conocidas de esta prueba no permiten decir inequívocamente, con seguridad (y con menos seguidad si no se tiene síntomas), que una persona sea inmune o no lo sea, y puede haber errores inadmisibles en los dos sentidos, a/ decir que una persona es inmune y no lo es (falso positivo) y b/ decir que no es inmune y que lo sea (falso negativo).
- Todo ello lo valoramos con la sensibilidad y la especificidad. A más sensibilidad, menos falsos negativos. A más especificidad, menos falsos positivos.
- Se intenta que ambas características, sensibilidad y especificidad, sean casi del 100%, pero en la práctica es difícil tal perfección, y por eso se suele seleccionar para las pruebas a grupos de población en que la infección es más probable.
- Para que te hagas idea, en las pruebas del SIDA la sensibilidad es del 99,5% y la especificidad es del 99,9% pero el resultado positivo de la prueba (estar infectado por el virus del SIDA, el VIH) es verdaderamente positivo sólo en la mitad de los casos (50%) cuando la prueba se hace en población de bajo riesgo, como mujeres donantes de sangre en que la probabilidad de la infección es muy baja, del 0,01%. Si se hace en un grupo de alta prevalencia, del 0,1%, el resultado positivo es verdaderamente positivo en el 91% de los casos.
- En el caso del nuevo coronavirus, en el estudio del Ministerio de Sanidad en toda España, se encontró que aproximadamente el 12% de la población de Madrid tenía inmuno-globulinas IgG anti SARS-CoV-2, pero el resultado es muy diferente según la edad, o según se haya tenido en el hogar a un paciente con COVID19 (“lo que es tu caso”) en que la prevalencia de tener IgG sube al 27%.
- Esto hay que tenerlo en cuenta para valorar el resultado de la determinación de los anticuerpos en personas asintomáticas.
- Si hay baja prevalencia, en personas asintomáticas, un resultado negativo casi con toda probabilidad es un verdadero negativo. Sin embargo, un resultado positivo en este mismo grupo sólo será verdaderamente positivo en algo más de la mitad (en torno al 60%). Al 40% restante (falsos positivos) se les diagnosticará y seguirá sin razón alguna.
- “¿Me sigues?”
- “Sí, mamá. Este virus es especial para todo y los anticuerpos no siempre aparecen en el orden ni en la fecha habitual. Y, además, los resultados no son ciertos al 100% pues hay siempre falsos positivos y falsos negativos. En un grupo de baja prevalencia, y en personas sin síntomas, casi todos los negativos serán verdaderos negativos, y entre los positivos sólo serán verdaderos positivos algo más de la mitad. Por ello conviene hacer la determinación de anticuerpos sólo cuando haya síntomas y sospecha clínica de COVID19. Y en todo caso en grupos de población con alta prevalencia de contacto con el virus”.
- “Bien, da gusto ver lo bien que lo entiendes. Sigo”.
- En medicina todo son probabilidades, ya te comenté el teorema de Bayes, y lo que hacemos es ir adquiriendo seguridad en el diagnóstico con las distintas “pruebas”, desde la historia clínica a la exploración física y las pruebas diagnósticas como análisis varios, radiología, etc. No es lo mismo hacerlo en persona con síntomas, que en asintomáticas.
- Además, aunque una persona fuera inmune no se puede asegurar que no contagie, en el sentido de ser o no ser “portador” sano del virus.
- Tampoco conocemos el tiempo de duración de la inmunidad, y hasta qué punto tener inmunidad implica no desarrollar la enfermedad.
- En todo caso, cuando hay sospecha de enfermedad, se procede a realizar la otra prueba, la PCR, con la que se busca directamente el virus en la mucosidad nasal (o en la saliva). A su vez, la PCR tiene sus problemas, “como ya te expliqué”, y más en personas sin síntomas.
-Jo, mamá, me dejas con la boca abierta. No entiendo porqué se están haciendo el análisis de anticuerpos a todo el mundo del sector educativo.
-Pues lo que está haciendo la Comunidad de Madrid es lo que llaman “pasaporte inmunitario o serológico”, que cuando lo anunció en general tuvo que retirarlo por las críticas, dados sus problemas científicos, éticos, legales y de justicia social.
-¿Nos han empleado de “conejillos de India”?
-Sí, eso. Con varios problemas: 1/ no se sabe con exactitud cuánto dura la efectividad de los anticuerpos generados en aquellos pacientes que ya se han expuesto al SARS-CoV-2 por lo que no es garantía de nada, 2/ las pruebas producen falsos positivos y falsos negativos en porcentajes que depende de la prevalencia de infección en los distintos grupos de población y 3/ si no se ha pedido consentimiento informado, ni se ha consensuado con claustros y sindicatos, se ha abusado de la buena fe de los trabajadores, y puede ser una medida estigmatizante y discriminatoria que conlleve problemas de protección de datos, libertad de circulación y derecho a la intimidad.
-Es un abuso, pues.
-Sí, sin duda. De hecho la determinación de anticuerpos en grupos y poblaciones sin síntomas tiene graves problemas científicos y no se suele recomendar salvo para estudios epidemiológicos y de salud pública.
-¿Y que hago yo, me hago la PCR…?
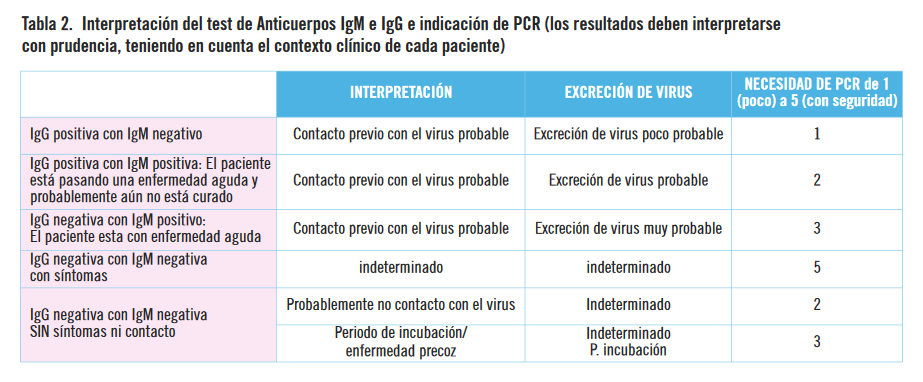
-Es raro el resultado tuyo, eso que sugiere infección aguda, pues no tienes síntomas. Lo más probable es que sea un resultado falso positivo. Echa un ojo a estas tablas, que te ayudarán a entender la situación. Fíjate que la recomendación de realizar la PCR está “graduada” y debería depender del criterio clínico no de una rutina sin más.
-Jo, me resulta increíble todo esto, déjame un momento para hacerme idea de lo que dicen las tablas.
-¿Entiendes las tablas?
-¡Mamá, que no soy analfabeta, y con lo que me has explicado ya tendría suficiente, pero las tablas son muy docentes! Ya veo que mi situación (IgM positiva, IgG negativa, sin síntomas) ni siquiera se considera.
-En todo caso, ve a las fuentes, a la bibliografía. Y por precaución, hazte la PCR y hasta que te den el resultado quédate en casa y conserva registro de con quien estás teniendo contacto.
-¡Jo, mamá, tú siempre con las “fuentes”! ¡Si no fuera por lo que me has explicado…!
-Vale, voy a preparar un té y nos lo tomamos mientras me cuentas del inicio del curso y sus problemas.
Mercedes Pérez-Fernández, Especialista en Medicina Interna, médico general jubilada, Equipo CESCA, Madrid, España mpf1945@gmail.com
Juan Gérvas, Doctor en Medicina, médico general jubilado, Equipo CESCA, Madrid, España jjgervas@gmail.com
Mercedes Pérez-Fernández y Juan Gérvas son miembros de NoGracias.
Bibliografía
-Antibody testing for coronavirus disease 2019: not ready for prime time
https://www.bmj.com/content/370/bmj.m2655
-Declaración del #siapCOVID19 sobre pasaportes serológicos
https://covid19siap.wordpress.com/declaracion-del-siapcovid19-sobre-pasaportes-serologicos/
-Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections
https://www.nature.com/articles/s41591-020-0965-6
-Comenzamos a realizar test de COVID-19 a alrededor de 100.000 docentes madrileños
-Estudio ENE-COVID: Informe final Estudio Nacional de Sero-epidemiología de la Infección por SARS-CoV-2 en España
https://www.mscbs.gob.es/ciudadanos/ene-covid/docs/ESTUDIO_ENE-COVID19_INFORME_FINAL.pdf
-Explicación de los distintos tests del covid-19
https://www.medmesafe.com/medicina-predictiva/explicacion-de-los-distintos-tests-del-covid-19
-HIV screening: helping clinicians make sense of test results to patients
https://www.bmj.com/content/347/bmj.f5151
-Información sobre el Coronavirus COVID-19: Diagnóstico
https://www.murciasalud.es/pagina.php?id=458263&idsec=5
-Indicaciones y procedimientos de tests diagnósticos de infección COVID19
https://www.saludcastillayleon.es/es/covid-19/informacion-profesionales/atencion-hospitalaria.ficheros/1582147-Indicaciones%20y%20procedimiento%20de%20utilizaci%C3%B3n%20de%20test%20diagn%C3%B3sticos%20de%20infecci%C3%B3n%20COVID-19-ACTUALIZADO%20%2815%20abril%29.pdf
-Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Serologic Testing
https://www.idsociety.org/practice-guideline/covid-19-guideline-serology/
-Interpretación de las pruebas diagnósticas frente a Sars-CoV-2
-¿Le ha dado positivo en la prueba del VIH de la farmacia?
http://saludineroap.blogspot.com/2018/01/le-ha-dado-positivo-en-la-prueba-del.html
-“Mamá, me van a hacer una PCR, la prueba del coronavirus. Y si me da positivo, ¿qué?”
-Overview of Testing for SARS-CoV-2 (COVID-19)
https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html
-Prevalencia de COVID-19: la clave para interpretar los test diagnósticos
http://saludineroap.blogspot.com/2020/04/prevalencia-de-covid-19-la-clave-para.html
-Symptoms and Testing: COVID-19
https://www.health.state.mn.us/diseases/coronavirus/symptoms.html
-Test diagnóstico COVID-19 en trabajadores de la salud asintomáticos
-What is the diagnostic accuracy of antibody tests for the detection of infection with the COVID-19 virus?
[English version]
“And now they have made me antibodies, Mom. It looks like an alphabet soup! » What does that mean for IgM positive and IgG negative and that PCR is recommended for me?».
There is a knock on the door and I will open it. She is my little daughter, agitated and distraught like never before. He comes in, he doesn’t take off his mask but he hugs me. Weird thing, he always removes his mask at home. It is an intense hug, as if the world was going to end. Cry I caress her back. He calms down and I can talk to him as we go into the living room and sit down.
-Daughter, there is nothing that worries me more than seeing you like this, broken.
-Mom, is that they have given me the result of the analysis that they have done to all the teachers, you know, and they say that now I have to do the PCR, that test that I only understood when you explained it to me.
-Yes. The thing about the Autonomous Community of Madrid has come out everywhere, about the endless queues. They say they want to test 100,000 education-related people as part of their strategy for a safe start to the 2020/21 course.
-Well, that. I didn’t want to bother you so I went when they summoned me and I was lucky to be among the first. But now they have given me the result and I am made a flan, I do not have it. I have tested positive for IgM and negative for IgG. And in this paper they have given us it literally says “Acute infection. You will receive a summons within 24 hours to carry out the PCR ”. -And they called you?
-Not. So I have tried calling where they did it to us without success. And they have not treated me in the health center, neither the nurse nor the doctor, the phone is blocked. That’s why I came to see you, unhinged, sorry. I can’t wait a day for them to call me. This is the best I have found on the internet.
-You can imagine how we are, they keep calling me colleagues asking me about what you wrote about the PCR! And in the groups there are all kinds of interpretations. It’s to go crazy! I don’t know who would think of it, but he screwed up.Do you notice anything, are you okay?
-Mother! I am like a rose, of course, yes, concerned with the beginning of the course and all the mess that nobody clears. You know, they had said that they were going to hire 11,000 new teachers and in the end there are only 300 and with the contract only until Christmas!
-They are scoundrels. But, and Jorge, is he also okay? As far as I know he was discharged and the PCR was negative, right?
-Yes, yes, he is very well since discharge, almost three weeks ago.
-And you have not had contact with anyone else who has been diagnosed or isolated by covid, is that correct?
-Yes, yes, with nobody-So, if you have not had contact with anyone infected and / or sick and if you are well (no fever, no cough, no shortness of breath, no cold, no loss of smell, no tiredness, no muscle pain, or anything at all ) it would be weird if you were infected. It is probably a false positive. Do you want me to explain it to you?
-Okay, yes, mom.
-There are several points in a row, if you understand the first one, you will surely understand the next one, and so on:
• Living things respond to infections in many ways, but one of them is with what people call “defenses”, antibodies
• Antibodies are proteins that we call immunoglobulins, hence the abbreviation for «Ig».
• Their structure is incredible, a wonder of Nature, but the fundamental thing is that they have a highly variable end, appropriate to each antigen (part of the germ that causes the formation of antibodies) and there are millions of different ends, and therefore millions of different antibodies, adapted to multiple antigens.
• When a person is infected with the new coronavirus, SARS-CoV-2, antibodies are produced to defend ourselves from infection (anti-SARS-CoV-2 immunoglobulins).
• Specific antibodies for the new coronavirus can be measured in the blood, taking a sample as they have done to you, with a technique we call ELISA and sometimes with other faster ones.
• The whole can be measured, total antibodies (Igt), or some more specific, A, M and G (immunoglobulins IgA, IgM, IgG). If there is a rush, the fastest and safest way is to measure total immunoglobulins (Igt).
• In general, IgM and IgG identification is preferred because there are fewer errors.
• IgM immunoglobulins are early-onset antibodies (shortly after infection, around 7 days after infection) and IgG immunoglobulins are late-onset antibodies (around 12 days after infection) and persistent over time (not known yet, but months in general).
• You already know how living beings are, so variable, so sometimes the production of antibodies is almost negligible, but there may be other defenses, such as those of T cells. In general, in people infected but who do not develop symptoms, who do not have the «florida» disease (they pass it, but it is inapparent), the production of antibodies is weaker and those antibodies last less time in the blood.
• «Are you following me?»
• «Yes mom. It is very simple, I have measured two antibodies in my blood against the coronavirus, immunoglobulins M and G, because they are the ones that give fewer errors. The M’s are the first to appear in the blood, and then the G’s. If I get infected and I have no symptoms, I produce fewer antibodies and they last less in the blood».
• «Okay, I’m going.»
• The new coronavirus is a special virus in a hundred ways, including that the antibody cadence is not as rigorously adhered to. In general, the IgMs are formed first, as an early response, and after a few days the IgGs are formed, but in this case it is not so clearly.
• Sometimes they cannot be determined in the blood until two weeks after the onset of symptoms, and the two immunoglobulins, IgM and IgG, rise at the same time, or the IgG even first increase.
• In the antibodies against the new coronavirus there is an inconsistency in the appearance of both classes of antibodies and it is a bit absurd to interpret IgM as «early», which is what is usually done in many other infections. That is why everything is more complicated, and even more so when there are no symptoms of disease or clinical suspicion of it so that the detection of antibodies ends up being totally useless.
• In general, however, it is often interpreted that a person who has antibodies has been infected by the virus, and 1 / if he has only early immunoglobulins (IgM), that he is in the early stages of infection, 2 / if you have both (IgM and IgG), that you are in an advanced infection phase, 3 / if you only have late immuno-globulins (IgG), that you have passed the infection and have defenses, and 4 / if you do not have any antibodies, or IgM or IgG, which has not had contact with the virus.
• This formation of antibodies occurs both in people who have had symptoms and the COVID19 disease and in people who have been infected and have overcome everything without giving any symptoms.
• In any case, you can imagine that there is no «exact» medical test, nor is there any scientific test that does not have its limitations.• That is, the test can give false results, in both directions, false positives and false negatives.
• Actually, the determination of antibodies is for diagnosis, when there are symptoms and clinical suspicion of disease, not for people without symptoms. And they are tests that have not yet been perfected in the clinical sense, and less in asymptomatic people.
• The known characteristics of this test do not allow to say unequivocally, with certainty (and with less certainty if there are no symptoms), that a person is immune or not, and there may be unacceptable errors in both senses, a / say that a person is immune and he is not (false positive) and b / say that he is not immune and that he is (false negative).
• We value all of this with sensitivity and specificity. The higher the sensitivity, the less false negatives. The more specific, the less false positives.
• It is intended that both characteristics, sensitivity and specificity, are almost 100%, but in practice such perfection is difficult, and therefore population groups in which infection is more likely are usually selected for testing.
• To give you an idea, in AIDS tests the sensitivity is 99.5% and the specificity is 99.9% but the positive result of the test (being infected with the AIDS virus, HIV) is truly positive only in half of the cases (50%) when the test is done in a low-risk population, such as blood donors in whom the probability of infection is very low, 0.01%. If done in a group with a high prevalence of 0.1%, the positive result is truly positive in 91% of cases.
• In the case of the new coronavirus, in the study of the Ministry of Health in Spain, it was found that approximately 12% of the population of Madrid had anti-SARS-CoV-2 IgG immunoglobulins, but the result is very different depending on the age, or depending on whether a patient with COVID19 has been kept at home («what is your case») in which the prevalence of having IgG rises to 27%.
• This must be taken into account to assess the result of the determination of antibodies in asymptomatic people.
• If there is low prevalence, in asymptomatic people, a negative result is almost in all probability a true negative. However, a positive result in this same group will only be truly positive in slightly more than half (around 60%). The remaining 40% (false positives) will be diagnosed and will continue for no reason• «Are you following me?».
• «Yes mom. This virus is special for everything and the antibodies do not always appear in the order or on the usual date. And, furthermore, the results are not 100% true as there are always false positives and false negatives. In a low prevalence group, and in people without symptoms, almost all the negatives will be true negatives, and among the positives only slightly more than half will be true positives. For this reason, it is advisable to perform the determination of antibodies only when there are symptoms and clinical suspicion of COVID19. And in any case in population groups with a high prevalence of contact with the virus».
• “Well, it’s nice to see how well you understand. I follow».
• In medicine everything is probabilities, I already mentioned Bayes’ theorem, and what we do is to acquire certainty in the diagnosis with the different «tests», from the medical history to the physical examination and diagnostic tests such as various analyzes, radiology , etc. It is not the same to do it in person with symptoms, than in asymptomatic.
• In addition, even if a person were immune, it cannot be guaranteed that they are not contagious, in the sense of being or not being a healthy “carrier” of the virus.
• We also do not know the duration of immunity, and to what extent having immunity implies not developing the disease.
• In any case, when there is suspicion of disease, the other test is carried out, PCR, with which the virus is searched directly in the nasal mucus (or in saliva). In turn, CRP has its problems, «as I already explained to you», and more in people without symptoms.
-Jo, mom, you leave me with my mouth open. I don’t understand why everyone in the education sector is being tested for antibodies-Well, what the Community of Madrid is doing is what they call an “immunological or serological passport”, which when it was announced in general had to be withdrawn due to criticism, given its scientific, ethical, legal and social justice problems-Have they used us as “guinea pigs”?
-If that. With several problems: 1 / it is not known exactly how long the effectiveness of the antibodies generated in those patients who have already been exposed to SARS-CoV-2, so it is not a guarantee of anything, 2 / the tests produce false positives and false negatives in percentages that depend on the prevalence of infection in the different population groups and 3 / if informed consent has not been requested, nor has consensus been reached with cloisters and unions, the good faith of the workers has been abused, and may be a stigmatizing and discriminatory measure that entails problems of data protection, freedom of movement and the right to privacy-It’s an abuse, well.
-Yes, definitely. In fact, the determination of antibodies in groups and populations without symptoms has serious scientific problems and is not usually recommended except for epidemiological and public health studies.
-What do I do, I do the PCR …?
-Your result is rare, that suggests acute infection, since you have no symptoms. Most likely it is a false positive result. Take a look at these tables, they will help you understand the situation. Note that the recommendation to perform CRP is «graduated» and should depend on clinical criteria, not just routine.
-Jo, I find all this incredible, give me a moment to get an idea of what the boards say.
-Do you understand the boards?
-Mom, I’m not illiterate, and with what you’ve explained to me I’d have enough, but the tables are very educational! I see that my situation (IgM positive, IgG negative, no symptoms) is not even considered.
-In any case, go to the sources, to the bibliography. And as a precaution, do the PCR and until you get the result stay home and keep a record of who you are having contact with.
-Jo, mom, you always with the «sources»! If it weren’t for what you explained to me …!
-Okay, I’m going to make some tea and we drink it while you tell me about the start of the course and its problems.
Mercedes Pérez-Fernández, Specialist in Internal Medicine, retired general practitioner, CESCA Team, Madrid, Spain mpf1945@gmail.com
Juan Gérvas, Doctor of Medicine, retired general practitioner, CESCA Team, Madrid, Spain jjgervas@gmail.com
Mercedes Pérez-Fernández y Juan Gérvas are members of NoGracias.
Bibliography
-Antibody testing for coronavirus disease 2019: not ready for prime time
https://www.bmj.com/content/370/bmj.m2655
-Declaration of # siapCOVID19 on serological passports
https://covid19siap.wordpress.com/declaracion-del-siapcovid19-sobre-pasaportes-serologicos/
-Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections
https://www.nature.com/articles/s41591-020-0965-6
-We began to test for COVID-19 to around 100,000 teachers from Madrid
-ENE-COVID Study: Final Report National Study of Sero-epidemiology of Infection by SARS-CoV-2 in Spain
https://www.mscbs.gob.es/ciudadanos/ene-covid/docs/ESTUDIO_ENE-COVID19_INFORME_FINAL.pdf
-Explanation of the different covid-19 tests
https://www.medmesafe.com/predictive-medicine/explicacion-de-los-distintos-tests-del-covid-19
-HIV screening: helping clinicians make sense of test results to patients
https://www.bmj.com/content/347/bmj.f5151
-Information about the Coronavirus COVID-19: Diagnosis
https://www.murciasalud.es/pagina.php?id=458263&idsec=5
-Indications and procedures for diagnostic tests for COVID19 infection
-Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Serologic Testing
https://www.idsociety.org/practice-guideline/covid-19-guideline-serology/
-Interpretation of diagnostic tests against Sars-CoV-2
-Have you tested positive for HIV from the pharmacy?
http://saludineroap.blogspot.com/2018/01/le-ha-dado-positivo-en-la-pruba-del.html
– “Mom, they are going to do a PCR, the coronavirus test. And if I test positive, what?»
-Overview of Testing for SARS-CoV-2 (COVID-19)
https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html
-Prevalence of COVID-19: the key to interpreting diagnostic tests
http://saludineroap.blogspot.com/2020/04/prevalencia-de-covid-19-la-clave-para.html
-Symptoms and Testing: COVID-19
https://www.health.state.mn.us/diseases/coronavirus/symptoms.html
-COVID-19 diagnostic test in asymptomatic health workers
– What is the diagnostic accuracy of antibody tests for the detection of infection with the COVID-19 virus?